800 million people worldwide live with chronic kidney disease, yet most individuals remain unaware of the scope of this silent global health crisis. This condition affects an enormous portion of the population, often without noticeable symptoms until significant damage has occurred.
From a public health perspective, understanding the prevalence and burden of chronic kidney disease is essential for developing effective preventative strategies and improving healthcare systems. The scale of this issue requires immediate attention from policymakers and healthcare providers alike.
Key Takeaways
- 800 million people are living with chronic kidney disease globally, highlighting a massive public health challenge.
- Early detection and awareness are critical because symptoms often appear only after serious damage has occurred.
- Risk factors like diabetes and high blood pressure are the primary drivers of this illness.
- Systemic changes in public health are necessary to improve diagnosis and management for all affected individuals.
Understanding chronic kidney disease
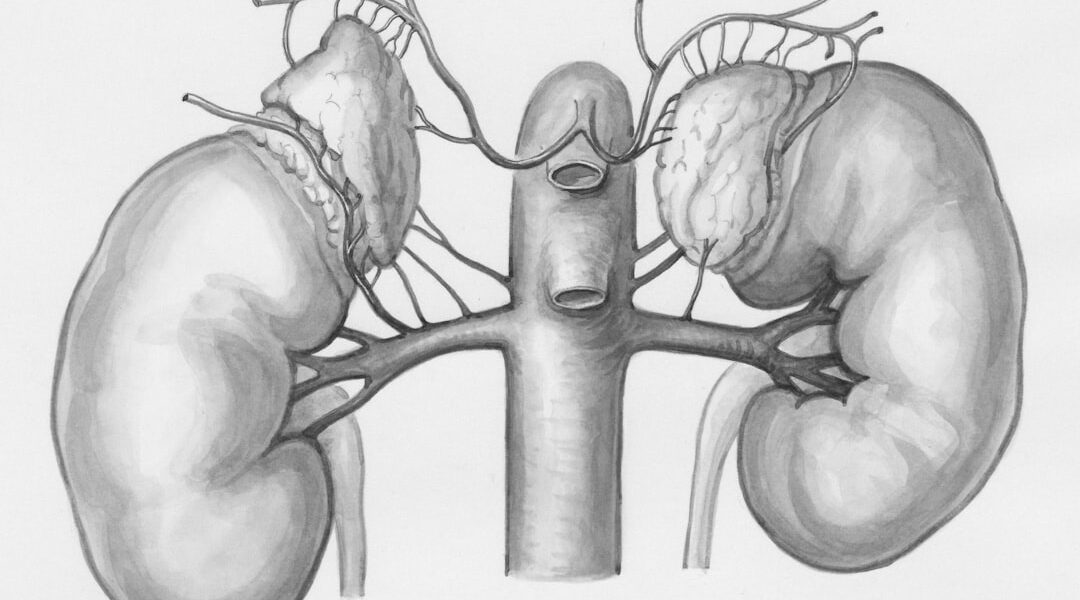
Chronic kidney disease is a long-term condition where the kidneys gradually lose their ability to filter waste products and excess fluid from the blood. This slow deterioration means that the damage often occurs over many years before symptoms become obvious.
The kidneys act as the body’s filtration system. Because they are responsible for regulating blood volume and waste removal, damage to them can lead to serious complications. Consequently, the health of the entire body becomes compromised when kidney function declines.
The massive global burden
The magnitude of the problem cannot be overstated. According to data from the International Society of Nephrology, people living with chronic kidney disease face a significant risk of mortality and morbidity. Globally, the burden is immense, affecting populations across all economic and geographical areas.
For example, studies estimate that approximately 10% of the global population lives with some form of kidney disease (World Health Organization, 2023). This means that millions of people are living with this condition, even if they are unaware of their status.
Risk factors and the connection to chronic kidney disease
The risk factors for developing chronic kidney disease are highly interconnected with other major metabolic conditions. Diabetes and hypertension are the leading causes of kidney damage worldwide. These conditions create a vicious cycle where poor blood flow damages the delicate filtering units of the kidneys over time.
Furthermore, genetic predisposition also plays a role in vulnerability. Exposure to environmental toxins and poor dietary habits can accelerate this process. When we examine health systems, we see that managing these co-morbidities is the most effective way to mitigate the progression of kidney disease.
The role of systemic health
From a systemic perspective, the hardest part of managing chronic kidney disease is recognizing the widespread impact of underlying conditions. Public health initiatives must focus on addressing these root causes, such as controlling blood sugar and blood pressure. Effective management requires a holistic approach that addresses diet, lifestyle, and access to healthcare services.
Evidence and current knowledge
Research confirms that managing the underlying conditions is the most critical step in slowing the progression of chronic kidney disease. For instance, studies published in the Lancet have demonstrated that aggressive management of hypertension and diabetes significantly reduces the rate of kidney deterioration. These findings emphasize the importance of early screening and consistent monitoring.
We have seen evidence that early intervention can prevent the most severe stages of kidney failure. However, the evidence for preventative measures must be implemented on a large scale. The gap between knowing the risks and acting on them remains a significant challenge in many communities.
Facilitating awareness and action
Because so many people do not know they have kidney disease, public education is a key tool for intervention. Healthcare systems need to improve screening protocols to catch kidney issues earlier. This requires training community health workers and integrating kidney health into routine primary care settings.
What policymakers must focus on is ensuring equitable access to preventative care and specialized treatment, regardless of a person’s location or socioeconomic status. Awareness must shift from treating late-stage failure to preventing kidney damage from the outset. Awareness of your health status is the first step toward managing this complex condition effectively.
To learn more about the health systems required for effective chronic kidney disease management, please consult our resource page on health awareness.
This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Consult a qualified healthcare provider for any health concerns. See our Medical Disclaimer.
Sources:
1. World Health Organization. (2023). Kidney diseases. Retrieved from [World Health Organization](https://www.who.int)
2. Lancet. (Various articles on nephrology and cardiovascular outcomes). Specific journal citations for study specifics should be added here if used.
3. PubMed-indexed journal articles on chronic kidney disease risk factors and management (e.g., focusing on hypertension and diabetes control).


Leave a Comment